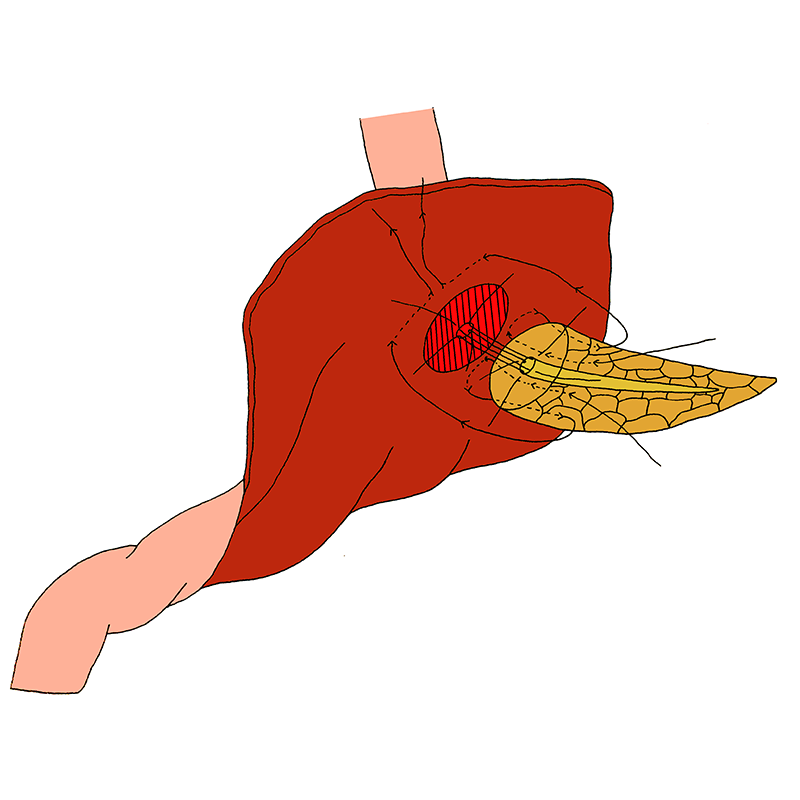
Duct-to-mucosa pancreatogastrostomy using a twin square wrapping method
- A seromuscular incision is made in the posterior gastric wall for a diameter that is similar to the diameter of the pancreatic stump.
- In the centre of the incised seromuscular layer, a 2 mm stab incision is carried out in the exposed gastric mucosa.
- The outer suture-row of the anastomosis consists of ‘twin square-shaped horizontal mattress and pancreas-transfixing sutures’, one on both side of the main pancreatic duct: these sutures are placed straight through the full-thickness of the pancreatic stump from posterior to anterior medially, then go horizontal (parallel to the width of the pancreatic remnant, from medial to lateral on both sides) through the seromuscular layer of the stomach wall, about 2 cm away from the seromuscular edge, and back through the pancreas from anterior to posterior laterally. The needles of both sutures are kept separately for later completion of the anastomosis.
- The inner suture-row consists of a duct-to-mucosa anastomosis, to which sutures are placed between the main pancreatic duct and the gastric mucosa circumferentially.
- For completion of the outer suture-line, the horizontal mattress sutures are continued and placed horizontally again, now from lateral to medial, through the seromuscular gastric layer, about 2 cm away from the seromuscular edge.
- Maemura K, Mataki Y, Kurahara H, et al. Pancreaticogastrostomy after pancreaticoduodenectomy using twin square wrapping with duct-to-mucosa anastomosis. Eur Surg Res. 2015;55:109-118