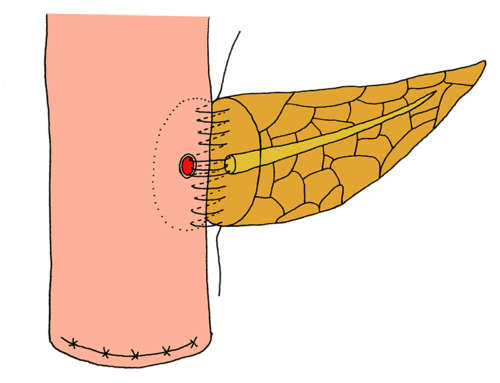
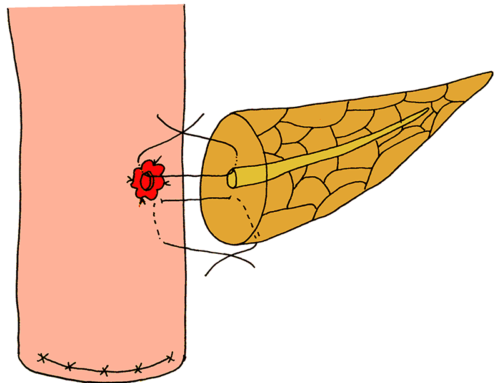
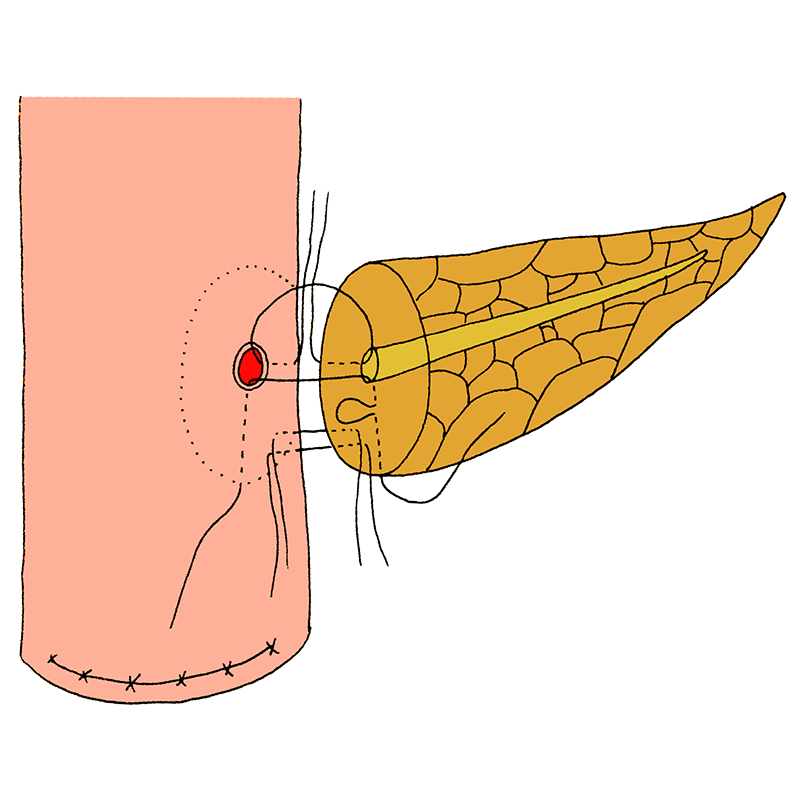
The pancreatic capsule is sutured to the seromuscular wall of the jejunum posteriorly, about 1 cm away from the pancreatic cut end. A small hole, with a diameter that matches the diameter of the main pancreatic duct, is made through the full-thickness of the jejunal wall, opposite to the pancreatic duct.
Whole-layer tightly appressed pancreatojejunostomy
- The pancreatic capsule is sutured to the seromuscular wall of the jejunum posteriorly, about 1 cm away from the pancreatic cut end.
- A small hole, with a diameter that matches the diameter of the main pancreatic duct, is made through the full-thickness of the jejunal wall, opposite to the pancreatic duct.
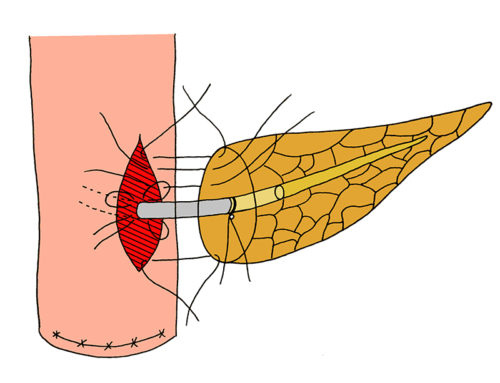
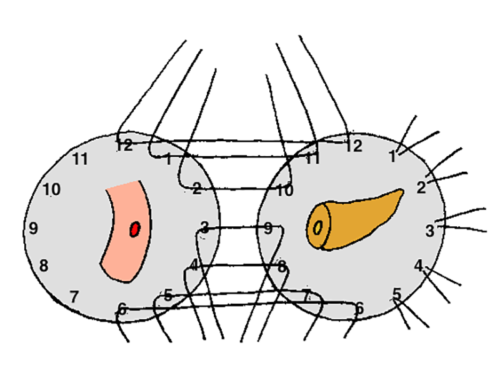
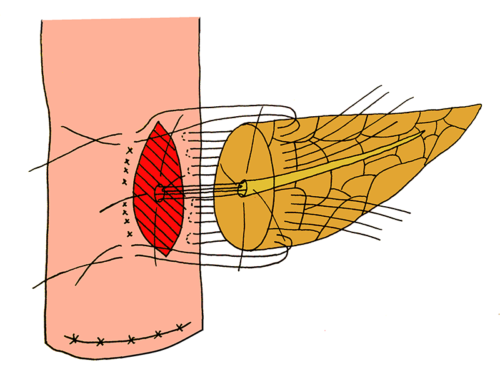
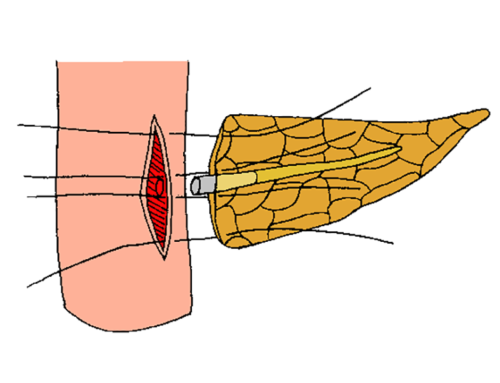
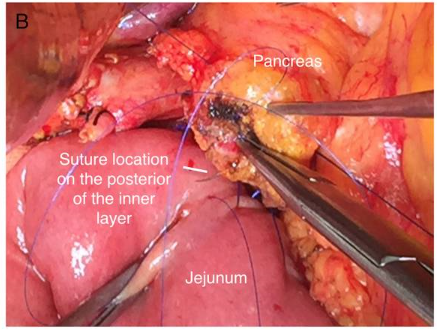
- A posterior inner suture-row is carried out between the pancreatic duct, including the complete pancreatic parenchyma, and the new-formed opening in the jejunum, including the full-thickness of the bowel wall. Suture-threads with a needle on both ends were used. The first needle of each suture is placed via the lumen of the main pancreatic duct, through the complete layer of pancreatic parenchyma, exiting the pancreas posteriorly from the pancreatic capsule. The second needle of each suture goes into the jejunal lumen, via the incision, and is pulled out through the full-thickness of the posterior jejunal wall.
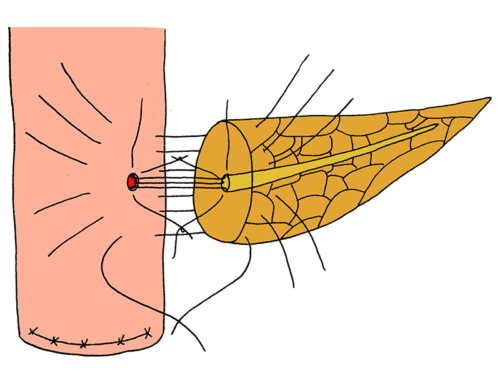
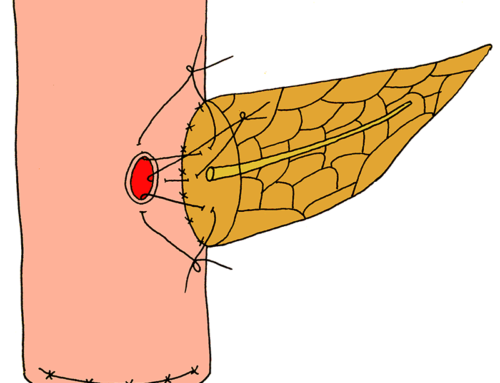
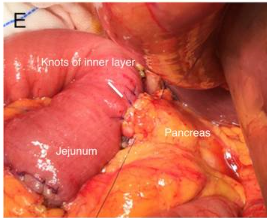
- The anterior inner suture-row is completed anteriorly in a same fashion as with the posterior inner suture-row.
- The pancreatic anastomosis is completed with an anterior outer suture-line between the pancreatic capsule and seromuscular jejunal wall.


- Zhang T, Wang X, Huo Z, et al. Shen’s whole-layer tightly appressed anastomosis technique for duct-to-mucosa pancreaticojejunostomy in pancreaticoduodenectomy. Med Sci Monit. 2016;22:540-548.