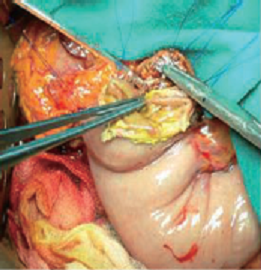
Before transection of the pancreas, two hemostatic sutures are placed cranially and caudally within the pancreatic parenchyma. After resection of the specimen, the anastomosis is started, using a double armed suture. For the first invagination stitch, the needle passed through the entire pancreatic remnant from anterior to posterior, 1 cm away from the cutting edge, cranially from the main pancreatic duct.
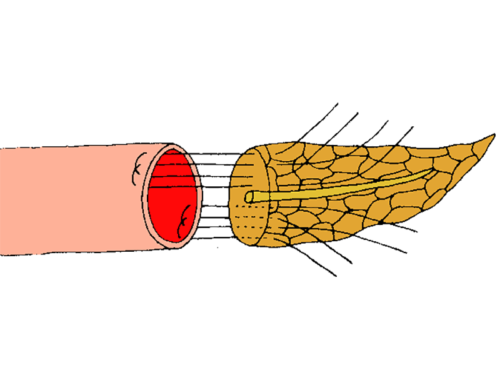
Transpancreatic invagination suturing technique
- Before transection of the pancreas, two hemostatic sutures are placed cranially and caudally within the pancreatic parenchyma.
- After resection of the specimen, the anastomosis is started, using a double armed suture. For the first invagination stitch, the needle passed through the entire pancreatic remnant from anterior to posterior, 1 cm away from the cutting edge, cranially from the main pancreatic duct. The needle is then placed through the posterior seromuscular layer of the jejunum, 1.5 cm away from the stapled end. Next, the needle is passed again through the entire pancreas – from posterior to anterior – a few millimeters next to the first stitch.
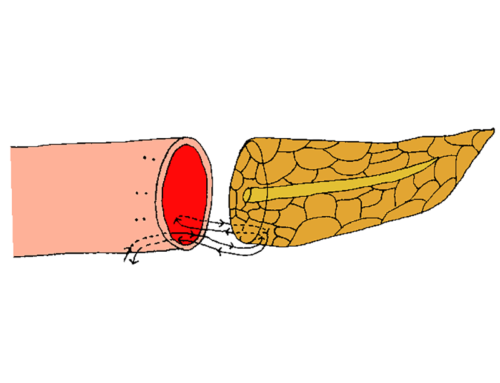
- A second invagination stitch is placed in a similar fashion, caudally from the main pancreatic duct. Both invagination sutures are kept separately.
- The two previously placed hemostatic sutures are placed through the seromuscular layer of the jejunum and tied. Herewith, the caudal and cranial cut margins of the pancreas are sutured together with the jejunal wall.
- Next, the metallic sutures in the stapled edge of the jejunum are removed, opening the transected jejunal loop.
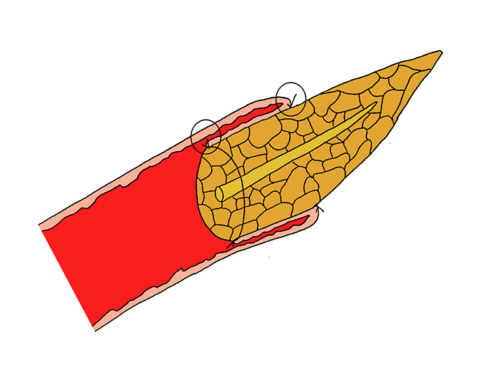
- For the inner suture line, the cut margins of pancreas and jejunum are sutured together circumferentially. This is done by the placement of interrupted stitches between the pancreatic capsula and seromuscular jejunal wall.
- After completing this internal layer of sutures, the two previously placed invaginating sutures are used to form the outer, inverting suture line. This is done by placing the needle through the anterior seromuscular layer of the jejunum, 1.5 cm away from the cut margin. The sutures are then tied with a single knot, causing invagination of the jejunum over the pancreas.
- To prevent compression of the pancreas, it is advised to loose the single knot after invagination of the jejunum and tying it thereafter with multiple knots.
- Care needs to be taken to avoid suturing through the main pancreatic duct. Furthermore, to avoid compression of the main pancreatic duct, an internal splint can be used.











- Giudici F, Pesi B, Zambonin D, Scaringi S, Bechi P, Batignani G. Safer intestinal invagination for a solid pancreatico-jejunal anastomosis in presence of a soft texture pancreatic remnant and non-dilated duct. Hepatobiliary Pancreat Dis Int. 2016;15:324-28.