The jejunal stump is everted for 3 cm, by suturing the jejunal free margin loosely to a point at the jejunal loop 6 cm from the cut edge. This leaves the mucosa exposed for excising. Mucosectomy of the everted part of the jejunum is applied. The pancreatic remnant is sutured to the mucosal margin of the jejunum in a circulair fashion.
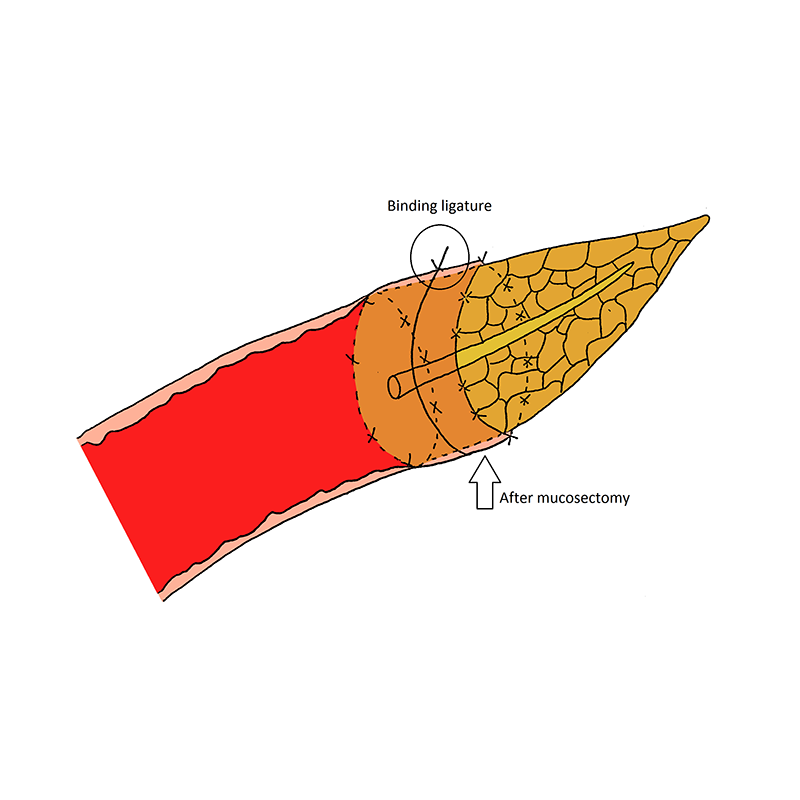
Binding pancreatojejunostomy
- The jejunal stump is everted for 3 cm, by suturing the jejunal free margin loosely to a point at the jejunal loop 6 cm from the cut edge. This leaves the mucosa exposed for excising. Mucosectomy of the everted part of the jejunum is applied.
- The pancreatic remnant is sutured to the mucosal margin of the jejunum in a circulair fashion. Care is taken to sew the mucosa only and avoid penetrating of the seromuscular layer of the jejunum. If possible, the pancreatic duct should be involved in the anterior or posterior suture-row.
- The everted jejunum is restored to its normal position by cutting the two loosely tied stitches. Now, the seromuscular layer of the jejunum forms a wrap around the pancreatic stump.
- A few stitches are placed to attach the cut margin of the jejunum to the pancreatic capsule.
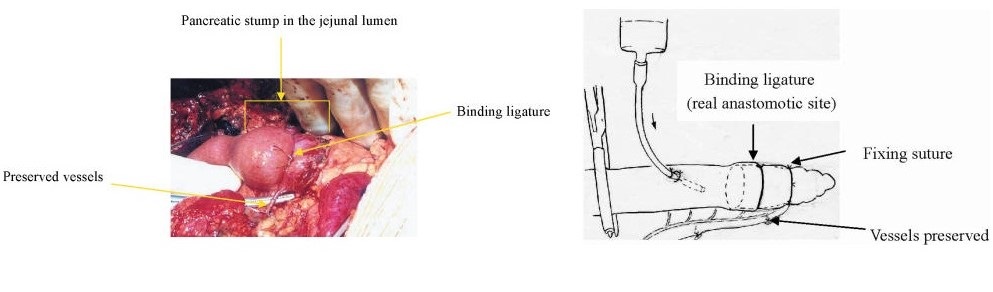
- Furthermore, an absorbable bond is looped around the entire circumference of the anastomosis, 1-2 cm from the cut edge of the jejunum, and tied until the two organs are in close contact with each other. Attention is paid to maintain adequate vasculature of the jejunum distal to the binding ligature. Also, the bond should not be tied too tight, to prevent atrophy of the pancreatic remnant and to preserve the patency of the main pancreatic duct.

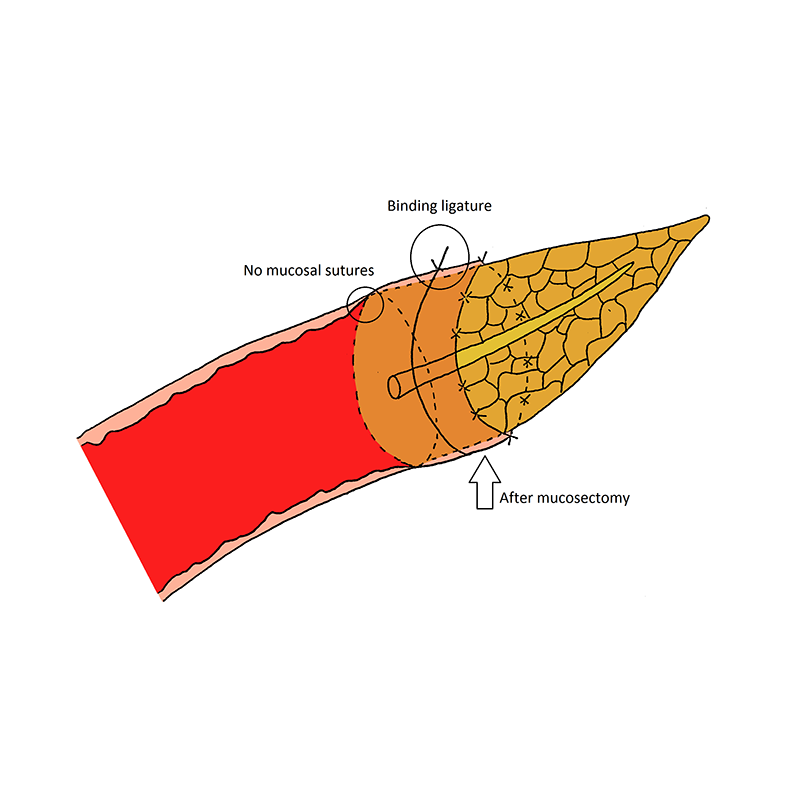
Type II binding pancreatojejunostomy
Type II binding pancreaticojejunostomy (modification): an alternative way to succeed the binding pancreatojejunostomy is without suturing the pancreatic cut edge to the jejunal mucosa. This technique is termed as type II binding pancreaticojejunostomy.
Binding pancreatojejunostomy
- Buc E, Flamein R, Golffier C, et al. Peng’s binding pancreaticojejunostomy after pancreaticoduodenectomy: a French prospective study. J Gastrointest Surg. 2010;14:705-710.
- Casadei R, Ricci C, Silvestri S, et al. Peng’s binding pancreaticojejunostomy after pancreaticoduodenectomy. An Italian, prospective, dual-institution study. Pancreatology. 2013;13:305-309.
- Kim JM, Hong JB, Shin WY, Choe YM, Lee GY, Ahn SI. Preliminary results of binding pancreaticojejunostomy. Korean J Hepatobiliary Pancreat Surg. 2014;18:21-25.
- Maggiori L, Sauvanet A, Nagarajan G, Dokmak S, Aussilhou B, Belghiti J. Binding versus conventional pancreaticojejunostomy after pancreaticoduodenectomy: a case-matched study. J Gastrointest Surg. 2010;14:1395-1400.
- Peng S, Mou Y, Cai X, Peng C. Binding pancreaticojejunostomy is a new technique to minimize leakage. Am J Surg. 2002;183:283-285.
- Peng SY, Mou YP, Liu YB, et al. Binding pancreaticojejunostomy: 150 consecutive cases without leakage. J Gastrointest Surg. 2003;7:898-900.
- Peng SY, Wang JW, Hong de F, Liu YB, Wang YF. Binding pancreaticoenteric anastomosis: from binding pancreaticojejunostomy to binding pancreaticogastrostomy. Updates Surg. 2011;63:69-74.
- Peng SY, Wang JW, Lau WY, et al. Conventional versus binding pancreaticojejunostomy after pancreaticoduodenectomy: a prospective randomized trial. Ann Surg. 2007;245:692-698.
- Peng SY, Wang JW, Li JT, Mou YP, Liu YB, Cai XJ. Binding pancreaticojejunostomy–a safe and reliable anastomosis procedure. HPB (Oxford). 2004;6:154-160.
Type II binding pancreatojejunostomy
