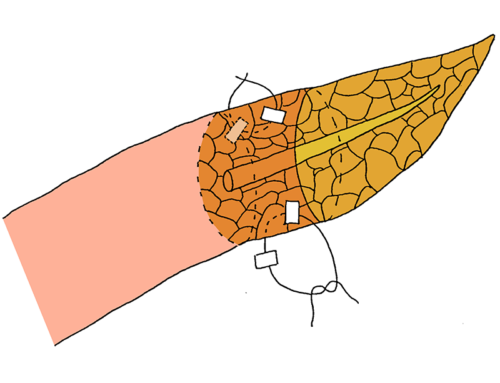
The pancreatic stump is invaginated into the jejunal lumen by two to three transpancreatic U-sutures, overlapping each other. The first U-suture is started at the mesenteric side of the anterior jejunum. This suture penetrates the jejunal wall from outside to inside about 1 cm distal to the cut edge and is then withdrawn from the jejunal opening.
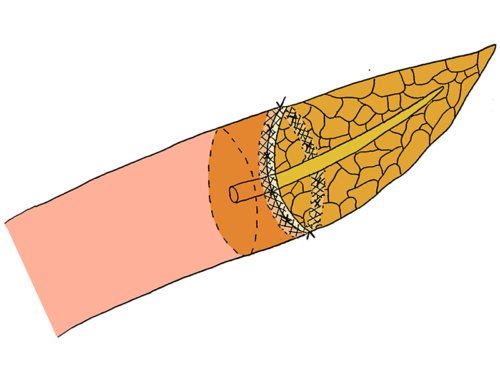
One-layered invagination end-to-end pancreatojejunostomy with overlapping transpancreatic U-sutures
- The pancreatic stump is invaginated into the jejunal lumen by two to three transpancreatic U-sutures, overlapping each other.
- The first U-suture is started at the mesenteric side of the anterior jejunum. This suture penetrates the jejunal wall from outside to inside about 1 cm distal to the cut edge and is then withdrawn from the jejunal opening. A front-to-back bite through the inferior pancreatic parenchyma is taken, approximately 1.5-2 cm from the cut surface. The needle is brought back into the jejunum via the jejunal opening and passed through the posterior jejunal wall to outside, at the mesenteric side. The suture is inserted into the jejunal loop again at the middle point of the posterior wall. The pancreatic parenchyma is penetrated in full-thickness from back to front at the midpoint between the superior and inferior edges. The first U-suture is completed, by inserting the needle from inside the jejunal lumen to outside through the midpoint of the anterior bowel wall.
- Until the remaining U-sutures have been performed, the first suture is not tied.
- The second U-suture is started, adjacent to the first U-suture, at the middle point of the anterior jejunal wall. After penetrating the jejunum from outside to inside, the needle is going straight through the full-thickness of the pancreas from front to back at the midpoint between the superior and inferior edges, close to the first U-suture. At the middle point of the posterior jejunal wall, the needle is placed to outside and inserted again at the superior edge of the posterior wall. Withdrawn from the jejunal opening, the superior edge of the pancreatic parenchyma is penetrated from front to back. Finally the suture is placed through the superior edge of the anterior bowel wall, from in- to outside.
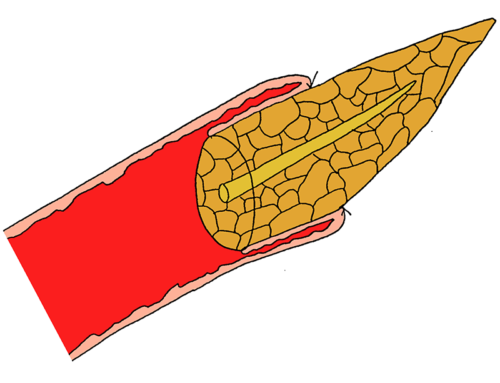
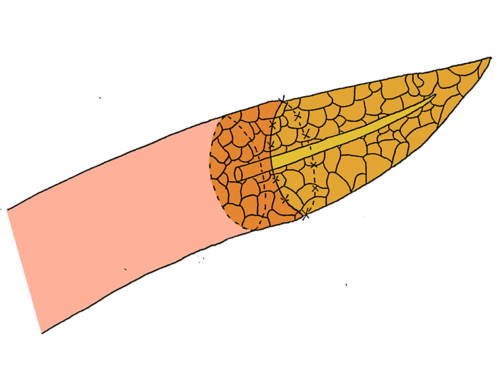
- After finishing the second suture, the double U-sutures are slowly strained by two surgeons at the same time and tied separately, resulting in invagination of the pancreas into the jejunal loop.
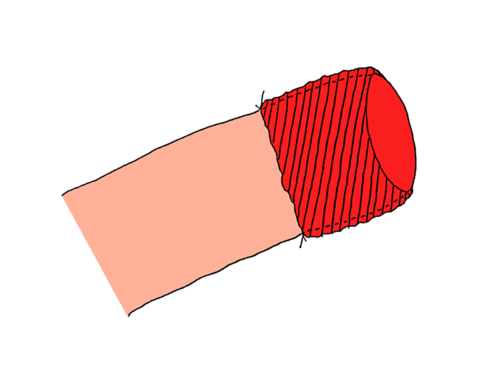
- The anastomosis is completed by the addition of four to six sutures between the seromuscular layer of the jejunal wall and the pancreatic capsule circumferentially.
- Binziad S, Salem AA, Amira G, Mourad F, Ibrahim AK, Manim TM. Impact of reconstruction methods and pathological factors on survival after pancreaticoduodenectomy. South Asian J Cancer. 2013;2:160-168.
- Chen XP, Huang ZY, Lau JW, et al. Chen’s U-suture technique for end-to-end invaginated pancreaticojejunostomy following pancreaticoduodenectomy. Ann Surg Oncol. 2014;21:4336-4341.
- Li T, Luo LX, Zhang C, et al. End-to-End Invaginated Pancreaticojejunostomy with Three Overlapping U-Sutures–A Safe and Simple Method of Pancreaticoenteric Anastomosis. J Invest Surg. 2015;28:115-119.
- Chen XP, Qiu FZ, Zhang ZW, Chen YF, Huang ZY, Zhang WG. A new simple and safe technique of end-to-end invaginated pancreaticojejunostomy with transpancreatic U-sutures–early postoperative outcomes in consecutive 88 cases. Langenbecks Arch Surg. 2009;394:739-744.