A seromuscular incision is made in the posterior gastric wall, with a size comparable to the diameter of the pancreatic remnant. A small mucosal incision in the centre of the incised seromuscular layer, opposite of the main pancreatic duct. An outer suture-line is performed between the anterior pancreatic capsule and the seromuscular cut edge of the posterior gastric wall first.
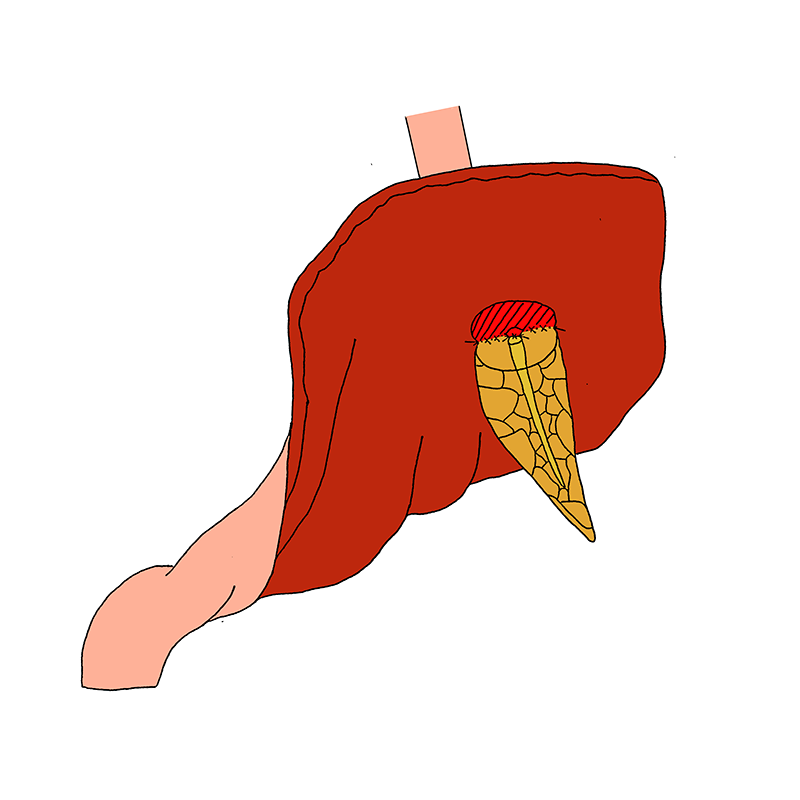
Duct-to-mucosa pancreatogastrostomy with seromuscular incision
- A seromuscular incision is made in the posterior gastric wall, with a size comparable to the diameter of the pancreatic remnant.
- A small mucosal incision in the centre of the incised seromuscular layer, opposite of the main pancreatic duct.
- An outer suture-line is performed between the anterior pancreatic capsule and the seromuscular cut edge of the posterior gastric wall first.
- Second, the main pancreatic duct is sutured circumferentially to the mucosa around the small opening in the posterior stomach wall to form the inner, duct-to-gastric-mucosa suture-row.
- The anastomosis is completed by finishing the outer suture-row between the posterior pancreatic capsule and the seromuscular cut edge of the posterior gastric wall.
Duct-to-mucosa pancreatogastrostomy without seromuscular incision
An alternative way to perform the duct-to-mucosa pancreatogastrostomy is without seromuscular incision in the posterior wall of the stomach. As a result, the small opening is made in the full-thickness of the stomach wall and. Sutures from the inner, duct-to-mucosa suture-row are now circumferentially placed between the main pancreatic duct and the full-thickness of the gastric wall. The remaining aspects of the anastomosis are carried out in a same way as described above.

With seromuscular incision
- Uemura K, Murakami Y, Sudo T, et al. Elevation of urine trypsinogen 2 is an independent risk factor for pancreatic fistula after pancreaticoduodenectomy. Pancreas. 2012;41:876-881
- Morris DM, Ford RS. Pancreaticogastrostomy: preferred reconstruction for Whipple resection. J Surg Res. 1993;54:122-125
- Murakami Y, Uemura K, Hayashidani Y, et al. No mortality after 150 consecutive pancreatoduodenctomies with duct-to-mucosa pancreaticogastrostomy. J Surg Oncol. 2008;97:205-209
- Murakami Y, Uemura K, Hayashidani Y, et al. Long-term pancreatic endocrine function following pancreatoduodenectomy with pancreaticogastrostomy. J Surg Oncol. 2008;97:519-522
- Murakami Y, Uemura K, Hayasidani Y, et al. A soft pancreatic remnant is associated with increased drain fluid pancreatic amylase and serum CRP levels following pancreatoduodenectomy. J Gastrointest Surg. 2008;12:51-56
- Murakami Y, Uemura K, Sudo T, et al. An antecolic Roux-en Y type reconstruction decreased delayed gastric emptying after pylorus-preserving pancreatoduodenectomy. J Gastrointest Surg. 2008;12:1081-1086
Without seromuscular incision
- Tomimaru Y, Takeda Y, Kobayashi S, et al. Comparison of postoperative morphological changes in remnant pancreas between pancreaticojejunostomy and pancreaticogastrostomy after pancreaticoduodenectomy. Pancreas. 2009;38:203-207
- Ihse I, Axelson J, Hansson L. Pancreaticogastrostomy after subtotal pancreatectomy for cancer. Dig Surg. 1999;16:389-392
- Conaglen PJ, Collier NA. Augmenting pancreatic anastomosis during whipple operation with fibrin glue: a beneficial technical modification? ANZ J Surg. 2014;84:266-269
- Payne RF, Pain JA. Duct-to-mucosa pancreaticogastrostomy is a safe anastomosis following pancreaticoduodenectomy. Br J Surg. 2006;93:73-77
- Telford GL, Mason GR. Pancreaticogastrostomy: clinical experience with a direct pancreatic-duct-to-gastric-mucosa anastomosis. Am J Surg. 1984;147:832-837